omeprazole
CLINICAL USE
Gastric acid suppressionDOSE IN NORMAL RENAL FUNCTION
Oral: 10–120 mg daily IV: 40 mg once daily for up to 5 days Patients with recent bleeding on endoscopy: 80 mg stat followed by 8 mg/hour for 72 hours (British Society of Gastroenterology)PHARMACOKINETICS
DOSE IN RENAL IMPAIRMENT
GFR (mL/MIN)
DOSE IN PATIENTS UNDERGOING RENAL REPLACEMENT THERAPIES
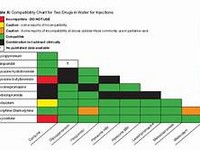
IMPORTANT DRUG INTERACTIONS
Potentially hazardous interactions with other drugsADMINISTRATION
Reconstition
5 mL solvent provided per 40 mg vialRoute
Oral, IVRate of Administration
Bolus: over 5 minutes Infusion: 40 mg over 20–30 minutes Continuous infusion: 8 mg/hourComments
Add to 100 mL sodium chloride 0.9% or glucose 5%Once diluted stable for 12 hours in sodium chloride 0.9% and 3 hours in glucose 5%Use oral as soon as possible 200 mg in 50 mL for 8 mg/hour infusion. (UK Critical Care Group, Minimum Infusion Volumes for fluid restricted critically ill patients, 3rd Edition, 2006)OTHER INFORMATION
Omeprazole clearance is not limited by renal disease.
See how to identify renal failure stages according to GFR calculation
See how to diagnose irreversible renal disease
Home