acute otitis media
acute otitis media
ESSENTIALS OF DIAGNOSIS
General Considerations
Acute otitis media is a bacterial infection of the mucosally lined air-containing spaces of the temporal bonePurulent material forms not only within the middle ear cleft but also within the pneumatized mastoid air cells and petrous apex
Acute otitis media is usually precipitated by a viral upper respiratory tract infection that causes eustachian tube obstruction
This results in accumulation of fluid and mucus, which becomes secondarily infected by bacteria
The most common pathogens are Streptococcus pneumoniae, Haemophilus influenzae, and Streptococcus pyogenes
Clinical Findings
Acute otitis media may occur at any agePresenting symptoms and signs include otalgia, aural pressure, decreased hearing, and often fever
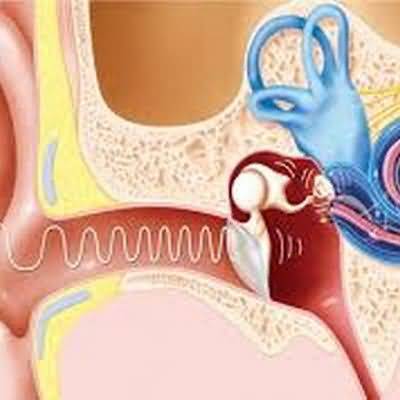
The typical physical findings are erythema and decreased mobility of the tympanic mem- brane (Figure 8–2)
Occasionally, bullae will appear on the tympanic membrane
Rarely, when middle ear empyema is severe, the tym- panic membrane bulges outward
In such cases, tympanic membrane rupture is imminent
Rupture is accompanied by a sudden decrease in pain, followed by the onset of otorrhea
With appropriate therapy, spontaneous healing of the tympanic membrane occurs in most cases
When perforation persists, chronic otitis media may develop
Mastoid tenderness often accompanies acute otitis media and is due to the presence of pus within the mastoid air cells
This alone does not indicate suppurative (surgical) mastoiditis
Frank swelling over the mastoid bone or the association of cranial neuropathies or central findings indicates severe disease requiring urgent care
Treatment
The treatment of acute otitis media is specific antibiotic therapy, often combined with nasal decongestantsThe first-choice oral antibiotic treatment is amoxicillin (80–90 mg/kg/day divided twice daily) (or erythromycin [50 mg/ kg/day]) plus sulfonamide (150 mg/kg/day) for 10 days
Alternatives useful in resistant cases are cefaclor (20–40 mg/kg/day) or amoxicillin-clavulanate (20–40 mg/kg/day)
Tympanocentesis for bacterial (aerobic and anaerobic) and fungal culture may be performed by any experienced physician
A 20-gauge spinal needle bent 90 degrees to the hub attached to a 3-mL syringe is inserted through the inferior portion of the tympanic membrane
Interposition of a pliable connecting tube between the needle and syringe permits an assistant to aspirate without inducing movement of the needle
Tympanocentesis is useful for otitis media in immunocompromised patients and when infection persists or recurs despite multiple courses of antibiotics
Surgical drainage of the middle ear (myringotomy) is reserved for patients with severe otalgia or when complications of otitis (eg, mastoiditis, meningitis) have occurred
Recurrent acute otitis media may be managed with long-term antibiotic prophylaxis
Single daily oral doses of sulfamethoxazole (500 mg) or amoxicillin (250 or 500 mg) are given over a period of 1–3 months
Failure of this regimen to control infection is an indication for insertion of ventilating tubes