rosiglitazone
CLINICAL USE
Type 2 diabetes mellitusDOSE IN NORMAL RENAL FUNCTION
4–8 mg daily in 1–2 divided dosesPHARMACOKINETICS
DOSE IN RENAL IMPAIRMENT
GFR (mL/MIN)
DOSE IN PATIENTS UNDERGOING RENAL REPLACEMENT THERAPIES
IMPORTANT DRUG INTERACTIONS
Potentially hazardous interactions with other drugsADMINISTRATION
Reconstition
–Route
OralRate of Administration
–Comments
–OTHER INFORMATION
Measure liver function prior to initiating therapy, and then at regular intervalsShould not be used in patients with heart failure or history of heart failure; incidence of heart failure is increased when rosiglitazone is combined with insulinShould not be used in patients with acute coronary syndrome. Patients should be closely monitored for signs of heart failureMay be associated with a small increased risk of cardiac ischaemia particularly in combination with insulin. The combination of rosiglitazone and insulin should be used only in exceptional cases, and under close supervisionRosiglitazone is contraindicated for co- administration with insulin in the UK but not in the USANot recommended for use in patients with ischaemic heart disease or peripheral arterial disease; in patients with history of ischaemic heart disease rosiglitazone should only be used after careful evaluation of the patient’s individual risk
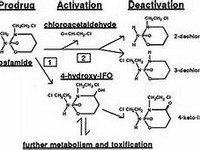
Rosiglitazone is extensively metabolised in the liver. Some of the metabolites are active, and are largely excreted in the urine.
See how to identify renal failure stages according to GFR calculation
See how to diagnose irreversible renal disease
Home