and microaneurysms but may also lead to reduced contrast sensitivity and retinal nerve fiber layer and outer retinal damage (HIV neuroretinal disorder)
CMV retinitis is less common since the availability of antiretroviral therapy (ART) but continues to be prevalent where resources are limited
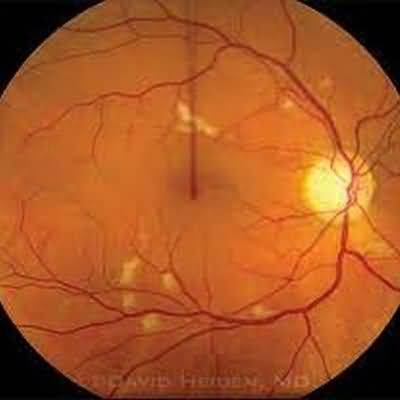
It usually occurs when CD4 counts are below 50/mcL (or 0
05 × 109/L) and is characterized by progressively enlarging yellowish-white patches of retinal opacification, accompanied by retinal hemorrhages, and usually beginning adjacent to the major retinal vascular arcades
Patients are often asymptomatic until there is involvement of the fovea or optic nerve, or until retinal detachment develops
Choices for initial therapy arevalganciclovir 900 mg orally twice daily for 3 weeksganciclovir 5 mg/kg intravenously twice a day, foscarnet 60 mg/kg intravenously three times a day, or cidofovir 5 mg/kg intravenously once weekly, for 2–3 weekslocal administration, using either intravitreal injection of ganciclovir or foscarnet, or the sustained-release ganciclovir intravitreal implant
All available agents are virostatic
Maintenance therapy can be achieved with lower-dose therapy (oral valganciclovir 900 mg once daily, intravenous ganciclovir 5 mg/kg/day, intravenous foscarnet 90 mg/kg/day, or intravenous cidofovir 5 mg/kg once every 2 weeks) or with intravitreal therapy
Systemic therapy has a greater risk of nonocular adverse effects but reduces mortality, incidence of nonocular CMV disease (but this is less common with ART), and incidence of retinitis in the fellow eye and avoids intraocular complications of intravitreal administration
Pharmacologic prophylaxis against CMV retinitis in patients with low CD4 counts or high CMV burdens has not been found to be worthwhile
In all patients with CMV retinitis, ART needs to be instituted or adjusted
This may lead to the immune reconstitution inflammatory syn- drome (IRIS), of which the immune recovery uveitis may lead to visual loss, predominantly due to cystoid macular edema
If the CD4 count is maintained above 100/mcL (0
1 × 109/L), it may be possible to discontinue maintenance anti-CMV therapy
Other ophthalmic manifestations of opportunistic infections occurring in AIDS patients include herpes simplex retinitis, which usually manifests as acute retinal necrosis; toxoplasmic and candidal chorioretinitis possibly progressing to endophthalmitis; herpes zoster ophthal- micus and herpes zoster retinitis, which can manifest as acute retinal necrosis or progressive outer retinal necrosis; and various entities due to syphilis, tuberculosis, or cryptococcosis
Kaposi sarcoma of the conjunctiva and orbital lymphoma may also be seen on rare occasions
Chronic HIV infection is associated with increased prevalence of age-related macular degeneration